Medical Disclaimer
This article provides evidence-based information about IV therapy research related to Chronic Fatigue Syndrome (CFS/ME). It is NOT medical advice. CFS is a complex, multi-system disease requiring specialized medical care. Always consult with your CFS specialist before starting any new treatment. Anyone promising to cure CFS is being dishonest—there is currently no cure.
Chronic Fatigue Syndrome (CFS), also known as Myalgic Encephalomyelitis (ME/CFS), is a debilitating multi-system disease characterized by profound fatigue that worsens after physical or mental exertion. With no cure currently available, patients and clinicians have explored various supportive therapies, including intravenous nutrient therapy.
This article examines what clinical research actually shows about IV therapy for CFS, reviews specific nutrient studies, sets realistic expectations, and provides practical guidance for patients considering IV therapy as part of their integrative care strategy.
Understanding CFS/ME: Core Symptoms and Diagnosis
CFS/ME is far more than ordinary tiredness. It's a complex, chronic illness that affects multiple body systems and significantly impacts quality of life[1].
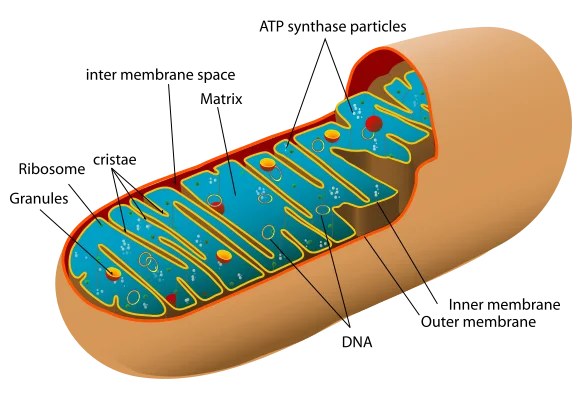
Mitochondria are the cellular powerhouses responsible for energy production. Mitochondrial dysfunction is a proposed mechanism in CFS/ME. Source: Wikimedia Commons, Public Domain
Core Diagnostic Criteria
- 1.Substantial reduction in activity level lasting more than 6 months, with profound fatigue that is not relieved by rest
- 2.Post-Exertional Malaise (PEM): Worsening of symptoms following physical, cognitive, or emotional exertion, often delayed 12-48 hours
- 3.Unrefreshing sleep: Waking up feeling exhausted despite adequate sleep duration
- 4.Cognitive impairment (brain fog) or orthostatic intolerance(symptoms worsen when standing)
Common Additional Symptoms
- - Muscle and joint pain without inflammation
- - Headaches of new type or severity
- - Sore throat, tender lymph nodes
- - Sensitivity to light, sound, chemicals
- - Temperature regulation problems
- - Gastrointestinal disturbances
Important Facts
- - Affects approximately 1-2.5 million Americans
- - More common in women (3:1 ratio)
- - Often begins after viral infection
- - No diagnostic laboratory test exists
- - Diagnosis is based on symptom criteria
- - No FDA-approved treatments available
Mitochondrial Dysfunction Theory
One leading hypothesis for CFS pathophysiology involves impaired mitochondrial function. Mitochondria are cellular powerhouses that produce ATP (adenosine triphosphate), the body's primary energy currency.
Research Findings
Multiple studies have documented mitochondrial abnormalities in CFS patients:
- Reduced ATP production: Research published in Clinical Sciencefound significantly lower ATP levels in CFS patients compared to healthy controls
- Oxidative stress: Increased markers of oxidative damage to mitochondria, documented in multiple studies
- Impaired electron transport chain: Dysfunction in Complex I and other components of cellular respiration
- Nutrient cofactor deficiencies: Many mitochondrial enzymes require B vitamins, magnesium, and CoQ10 as cofactors
Why This Matters for IV Therapy
If mitochondrial dysfunction contributes to CFS symptoms, then addressing nutrient cofactor deficiencies might theoretically support energy production. This is the rationale behind IV nutrient therapy—delivering therapeutic doses of B vitamins, magnesium, and other mitochondrial cofactors directly into the bloodstream. However, it's crucial to understand this is supportive care, not disease-modifying treatment.
B12 and CFS: What the Research Shows
Vitamin B12 (cobalamin) is essential for red blood cell formation, neurological function, and DNA synthesis. Several studies have examined B12 supplementation for CFS.
Japanese Study: Intramuscular B12
Results: Approximately 50-80% of patients reported symptom improvement, particularly in cognitive function and general well-being. However, the study lacked a placebo control group.
Interpretation: While promising, placebo response rates in CFS studies can reach 40-50%, making uncontrolled studies difficult to interpret.
Functional B12 Deficiency
Some CFS patients have normal serum B12 levels but elevated methylmalonic acid (MMA) and homocysteine—markers of functional B12 deficiency at the cellular level.
In these cases, high-dose B12 (especially methylcobalamin or hydroxocobalamin) may improve symptoms by addressing the functional deficiency that standard testing misses.
IV vs. IM vs. Oral B12
| Route | Bioavailability | Peak Levels | Best For |
|---|---|---|---|
| Oral | 1-5% (intrinsic factor dependent) | Low | Maintenance, mild deficiency |
| IM Injection | ~100% | High, sustained | Standard treatment for deficiency |
| IV Drip | ~100% | Very high, immediate | Rapid delivery with other nutrients |
Clinical Bottom Line
B12 supplementation (IV, IM, or high-dose oral) may benefit CFS patients with documented or functional B12 deficiency. Response is highly individual. Testing MMA and homocysteine can help identify functional deficiency. Do not expect B12 alone to dramatically resolve CFS.
Magnesium Studies in CFS
Magnesium is a cofactor in over 300 enzymatic reactions, including those involved in ATP synthesis. Several studies suggest magnesium deficiency may be common in CFS.
Red Blood Cell Magnesium Deficiency
Cox et al. (1991), The Lancet: Researchers measured red blood cell (RBC) magnesium in 20 CFS patients and 20 controls. Results showed significantly lower RBC magnesium in CFS patients, even when serum magnesium was normal.
Treatment Protocol:
Patients received 1g magnesium sulfate IM weekly for 6 weeks. 12 of 15 patients (80%) reported improved energy levels, reduced pain, and better emotional state. Only 3 of 17 placebo patients (18%) reported improvement.
Magnesium Functions in Energy Production
- - Required for ATP synthesis in mitochondria
- - Activates enzymes in glycolysis
- - Stabilizes ATP-magnesium complex
- - Regulates calcium channels (muscle function)
- - Reduces oxidative stress
- - Supports neurotransmitter production
Why Serum Levels Miss Deficiency
Less than 1% of total body magnesium is in serum. The body tightly regulates serum levels by pulling magnesium from bone and tissue stores.
Better test: RBC magnesium or ionized magnesium, though these aren't routinely available in all labs.
IV Magnesium for CFS
IV magnesium (typically magnesium sulfate or magnesium chloride) bypasses intestinal absorption limitations and rapidly restores cellular levels. Common in Myers Cocktail formulations.
Typical dose: 1-2 grams magnesium sulfate or chloride per infusion. Patients often report muscle relaxation, reduced pain, and improved sleep. Effects are usually temporary (days to weeks), requiring regular treatments for sustained benefit.
Coenzyme Q10 and Energy Production
Coenzyme Q10 (CoQ10, ubiquinone) is a crucial component of the mitochondrial electron transport chain. It's essential for ATP production and also functions as an antioxidant.
Maes et al. (2009): CoQ10 Deficiency in CFS
This study found significantly lower CoQ10 levels in CFS patients compared to healthy controls. Lower CoQ10 correlated with greater fatigue severity and more cognitive symptoms.
Supplementation trial: 150-300mg oral CoQ10 daily for 3 months showed modest improvements in fatigue scores in some patients, though results were mixed.
CoQ10 in Mitochondria
- - Electron carrier in Complex I and II
- - Essential for oxidative phosphorylation
- - Potent antioxidant (protects mitochondrial membrane)
- - Regenerates vitamin E
IV vs. Oral CoQ10
Oral: Fat-soluble, requires food for absorption. Ubiquinol form (reduced CoQ10) better absorbed than ubiquinone.
IV: Not commonly available in standard IV formulations. Most IV clinics use oral supplementation instead.
Clinical Consideration
While CoQ10 shows theoretical promise for mitochondrial support, clinical trials show only modest, inconsistent benefits. Some patients respond well; others notice no change. Oral supplementation (200-400mg/day ubiquinol) is typically tried before IV therapy.
Myers Cocktail for CFS: The Evidence
The Myers Cocktail is an IV nutrient formula containing magnesium, calcium, B vitamins (B12, B5, B6, B-complex), and vitamin C. It's one of the most commonly used IV therapies for CFS.
Ali et al. (2009): Placebo-Controlled Pilot Study
Published in the Journal of Alternative and Complementary Medicine, this small study evaluated IV micronutrient therapy (similar to Myers Cocktail) for fibromyalgia and CFS.
Protocol:
Weekly IV infusions for 8 weeks containing magnesium chloride, calcium gluconate, hydroxocobalamin, B vitamins, and vitamin C.
Results:
Modest improvement in quality of life scores and symptom severity compared to placebo. Benefits were statistically significant but clinically modest. Most patients did not experience dramatic improvement.
Important limitation: Small sample size (34 patients). Larger trials needed to confirm findings.
Dr. Alan Gaby's Clinical Experience
Dr. Alan Gaby, who refined the Myers Cocktail, documented outcomes in hundreds of patients over decades, including many with CFS. In his clinical review published inAlternative Medicine Review (2002), he noted:
- - Approximately 50-70% of CFS patients reported some benefit
- - Response was usually partial, not complete symptom resolution
- - Benefits lasted days to weeks, requiring regular treatments
- - Best results in patients with documented nutrient deficiencies
| Ingredient | Typical Dose | Proposed Mechanism in CFS |
|---|---|---|
| Magnesium Chloride | 1-2 grams | ATP synthesis, muscle relaxation, pain reduction |
| Vitamin B12 | 1,000-5,000 mcg | Energy metabolism, neurological function |
| B-Complex | 1-2 mL | Mitochondrial cofactors, neurotransmitter synthesis |
| Vitamin C | 2-10 grams | Antioxidant, immune support, adrenal function |
| Calcium Gluconate | 100-200 mg | Muscle contraction, nerve transmission |
Realistic Expectations: IV Therapy is Supportive, Not Curative
Critical Reality Check
There is no cure for CFS/ME. Any practitioner claiming IV therapy will cure CFS is being dishonest and potentially exploiting vulnerable patients.
IV nutrient therapy is supportive care that may help address specific deficiencies or provide modest symptom relief in some patients. It does not treat the underlying disease mechanism.
Realistic Benefits (Some Patients)
- - Modest reduction in fatigue severity (not elimination)
- - Temporary energy boost lasting hours to days
- - Reduced muscle pain and tension
- - Improved hydration status
- - Better sleep quality in some cases
- - Slight improvement in cognitive clarity
Unrealistic Expectations
- - Complete resolution of CFS symptoms
- - Cure or permanent remission
- - Ability to return to pre-illness activity levels
- - Dramatic, life-changing transformation
- - Long-lasting benefits from single treatment
- - Replacement for pacing and energy management
What the Research Actually Shows
Pacing and Energy Management: The Most Evidence-Based Strategy
While IV therapy remains experimental with modest evidence, pacing is the most well-supported management strategy for CFS. IV therapy should complement, not replace, proper energy management.
What is Pacing?
Pacing is the systematic management of activity to stay within your "energy envelope"— the amount of physical and mental exertion you can handle without triggering Post-Exertional Malaise (PEM).
Core Principles:
- 1. Break activities into smaller chunks with rest periods between
- 2. Stop before you feel tired (before hitting your energy limit)
- 3. Plan rest days between more demanding activities
- 4. Avoid boom-and-bust cycles (overdoing it on good days)
- 5. Prioritize essential activities and delegate or skip non-essential tasks
- 6. Monitor and adjust based on symptom response
Physical Pacing
- - Limit walking distance
- - Use mobility aids if needed
- - Sit while cooking, showering
- - Spread tasks across days
Cognitive Pacing
- - Limit screen time
- - Break work into 15-30 min blocks
- - Avoid multitasking
- - Rest brain between tasks
Social/Emotional Pacing
- - Limit social event duration
- - Say no without guilt
- - Rest before and after events
- - Choose low-stimulation activities
Why Pacing Matters More Than IV Therapy
No amount of IV therapy can compensate for consistently exceeding your energy envelope. PEM can set you back days, weeks, or even months. Pacing prevents PEM and stabilizes symptoms.
Evidence: Multiple studies show that activity pacing reduces symptom severity, improves function, and prevents crashes more effectively than push-through approaches or treatments alone. Consider IV therapy as one tool in a comprehensive management plan that centers on pacing.
Traveling to Bali with CFS: Practical Considerations
International travel with CFS requires careful planning and energy management. Bali can be accessible with the right strategies.
Pre-Travel Planning
- Flight strategy: Consider breaking long journeys with stopover, book aisle seats for easier movement, request wheelchair assistance if needed
- Accommodation: Choose quiet areas (Ubud, Sanur over Seminyak/Canggu), ground-floor rooms, close to amenities
- Medical preparation: Bring all medications, medical documentation, research local healthcare options
- Travel insurance: Ensure CFS/pre-existing conditions covered
During Your Stay
- Pacing: Schedule rest days between activities, plan half-days not full days
- Climate: Avoid midday heat (11am-3pm), stay hydrated, use AC for rest
- Food safety: Avoid Bali belly (compounds fatigue), stick to reputable restaurants
- Transport: Use private drivers instead of scooters, limit travel distances
How Mobile IV Therapy Can Support Travel
Mobile IV services in Bali can provide convenient support without requiring travel to a clinic:
- Post-flight recovery: Hydration + B vitamins can help with jet lag and travel fatigue
- Illness management: If you develop Bali belly or respiratory infection, IV fluids prevent dehydration
- Energy support: Myers Cocktail or B12 for modest energy boost on important days
- Convenience: Treatment comes to your villa—no energy spent traveling to clinic
Important Reminder
IV therapy cannot override poor pacing. If you overexert in Bali and trigger severe PEM, IV therapy won't rescue you. Respect your energy limits first; use IV support as needed for hydration, nutrient deficiencies, or illness recovery.
When IV Therapy May Help vs. When to Avoid
IV Therapy May Be Appropriate When:
- Documented deficiencies: Lab-confirmed low B12, magnesium, or other nutrients
- Functional deficiency: Normal serum levels but elevated MMA/homocysteine
- Absorption issues: GI symptoms preventing adequate oral intake
- Acute illness: Dehydration from Bali belly, respiratory infection requiring fluids
- Part of integrative plan: Combined with pacing, sleep hygiene, medical management
- Realistic expectations: You understand it's supportive, not curative
Avoid IV Therapy When:
- Promised cure: Provider claims IV will cure CFS (major red flag)
- Normal nutrient levels: No documented deficiency and no symptoms suggesting one
- Severe PEM: Currently crashed from overexertion (rest first, IV won't reverse it)
- Financial strain: IV therapy is expensive; doesn't make sense to go into debt
- Underlying conditions: Kidney disease, heart failure, or other contraindications
- Replacing proven strategies: Using IV as excuse to skip pacing, sleep hygiene
Questions to Ask Before Starting IV Therapy
Frequently Asked Questions
Can IV therapy cure Chronic Fatigue Syndrome?
No. There is currently no cure for CFS/ME. IV therapy is supportive, not curative. It may help address specific nutrient deficiencies that can worsen symptoms, but it does not treat the underlying disease mechanism. Anyone promising a CFS cure is being dishonest.
What nutrients are most studied for CFS?
The most studied nutrients for CFS include Vitamin B12 (especially methylcobalamin), magnesium (often deficient in CFS patients), Coenzyme Q10 (for mitochondrial support), and various B-complex vitamins. Small studies show modest improvements in some patients, but results are inconsistent.
How does B12 help with chronic fatigue?
B12 is essential for red blood cell production, nerve health, and energy metabolism. Some CFS patients have functional B12 deficiency despite normal serum levels. IV B12 (especially methylcobalamin) bypasses absorption issues and may improve energy in deficient individuals, though response varies significantly.
Is Myers Cocktail effective for CFS?
A small placebo-controlled pilot study suggested Myers Cocktail may provide modest symptom relief for some CFS patients, possibly due to magnesium and B-vitamin content. However, large-scale clinical trials are lacking. It's considered supportive therapy, not a primary treatment.
Can I travel to Bali with CFS?
Travel with CFS requires careful planning and energy management. Consider shorter flights with stopovers, pre-booking accommodations close to activities, planning rest days between excursions, and avoiding overscheduling. Mobile IV therapy can provide hydration and nutrient support during your stay if needed.
What is pacing and why is it important for CFS?
Pacing is the systematic management of activity to stay within your energy envelope and avoid post-exertional malaise (PEM). It involves breaking activities into smaller chunks, scheduling rest periods, monitoring energy levels, and stopping before you feel exhausted. It's the most evidence-based CFS management strategy.
When might IV therapy help with CFS symptoms?
IV therapy may provide modest support when there are documented nutrient deficiencies (B12, magnesium, etc.), during illness recovery requiring hydration, for severe gastrointestinal symptoms affecting oral intake, or as part of integrative care. It works best alongside pacing, sleep hygiene, and medical management.
When should I avoid IV therapy for CFS?
Avoid IV therapy if you have documented normal nutrient levels without symptoms of deficiency, are being promised a cure (major red flag), are experiencing severe PEM from recent overexertion (rest first), or have underlying conditions that make IV therapy risky. Always consult your CFS specialist before starting IV treatments.
IV Support Available in Bali
If you're managing CFS while visiting Bali and need supportive IV therapy for hydration, documented deficiencies, or illness recovery, our licensed medical team provides safe, professional service delivered to your location.
We provide honest, evidence-based care. We will never promise to cure CFS. IV therapy is supportive only and works best alongside proper pacing and medical management.
Scientific References
- [1] Fukuda K, et al. (1994). "The chronic fatigue syndrome: a comprehensive approach to its definition and study." Annals of Internal Medicine, 121(12), 953-959.PubMed
- [2] Myhill S, et al. (2009). "Chronic fatigue syndrome and mitochondrial dysfunction." International Journal of Clinical and Experimental Medicine, 2(1), 1-16.PubMed
- [3] Castro-Marrero J, et al. (2015). "Effect of coenzyme Q10 plus nicotinamide adenine dinucleotide supplementation on maximum heart rate after exercise testing in chronic fatigue syndrome." Clinical Nutrition, 35(4), 826-834.PubMed
- [4] Regland B, et al. (2015). "Response to vitamin B12 and folic acid in myalgic encephalomyelitis and fibromyalgia." PLoS One, 10(4), e0124648.PubMed
- [5] Gaby AR. (2002). "Intravenous nutrient therapy: the Myers cocktail." Alternative Medicine Review, 7(5), 389-403.PubMed
Related Articles
Myers Cocktail Guide
Complete breakdown of ingredients, benefits, and clinical research
Vitamin B12 for Energy
Understanding B12 deficiency, testing, and IV supplementation
IV Therapy Myths Debunked
Separating evidence-based facts from marketing claims
When NOT to Get IV Therapy
Contraindications, risks, and situations to avoid IV treatment