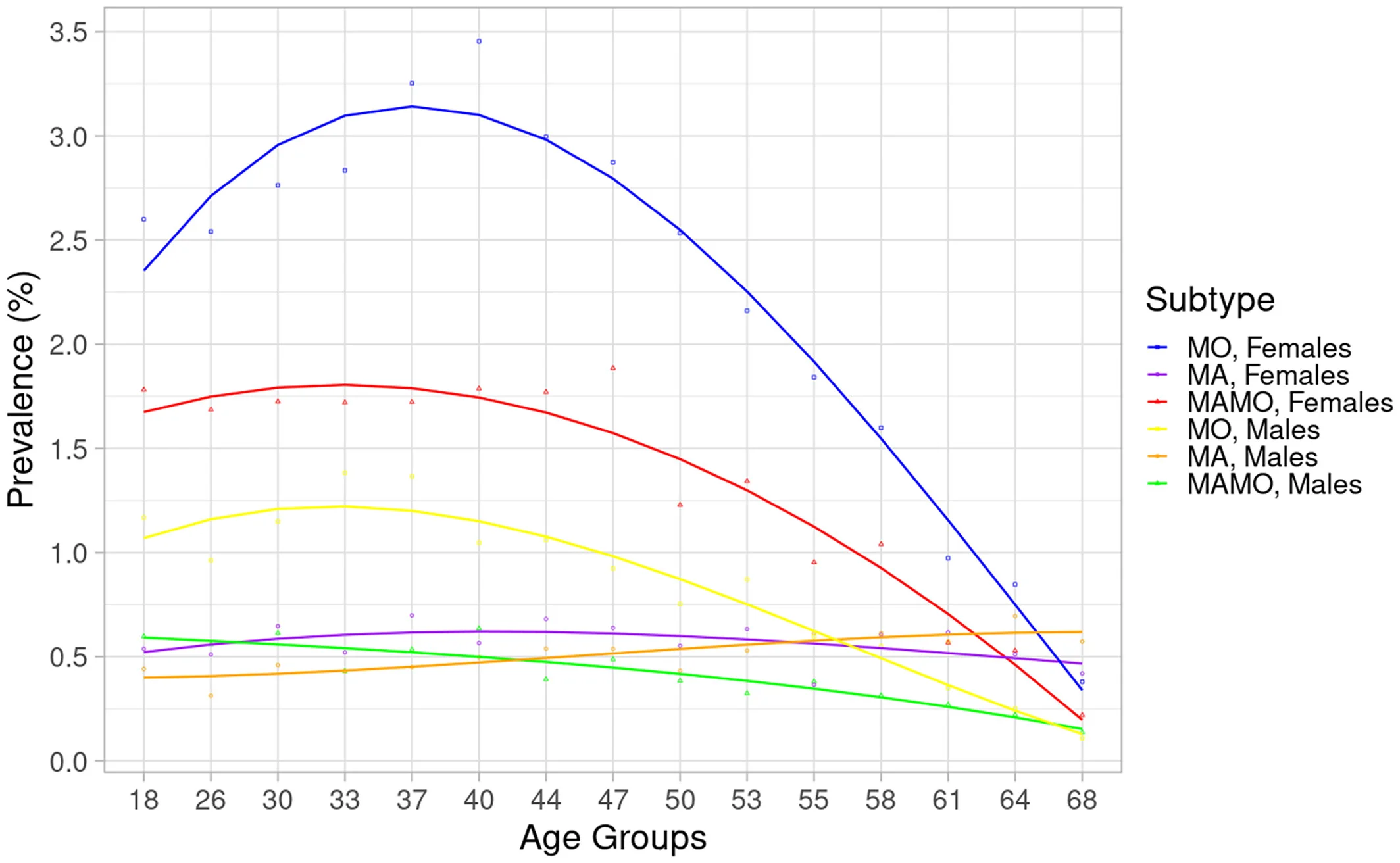
Migraine is a neurological condition that can be triggered by dehydration and nutrient deficiencies in tropical climates. Source: Wikimedia Commons
Migraine Triggers in Bali: Climate, Dehydration, and Jet Lag
If you're experiencing migraines in Bali for the first time, or noticing your usual migraines are more frequent here, you're not imagining it. Bali's tropical environment creates a perfect storm of migraine triggers that even people without a history of migraines can experience.
Understanding these environmental factors is crucial for both prevention and treatment. Let's break down the specific challenges Bali's climate presents for migraine sufferers.
Heat and Vasodilation
Bali's consistent 30-33 degrees Celsius temperatures cause blood vessels to dilate (expand) as your body attempts to cool itself. For migraine sufferers, vasodilation is a well-documented trigger. Research published in Neurology journal found that for every 5 degrees Celsius increase in temperature, migraine risk increases by 7.5%.
The heat effect is compounded by humidity. Bali's 70-85% humidity makes it harder for your body to cool through sweat evaporation, keeping those blood vessels dilated longer and increasing migraine susceptibility.
Dehydration: The Silent Trigger
In tropical climates, you lose significantly more fluid through perspiration than you might realize. Studies show that even mild dehydration (1-2% body weight loss) can trigger migraines in susceptible individuals.
The mechanism is two-fold:
- Blood volume reduction: Dehydration decreases blood volume, which reduces oxygen delivery to the brain, triggering migraine pathways
- Electrolyte imbalance: Sweating depletes magnesium and other electrolytes critical for preventing migraines
A study in The Journal of Clinical Neurology found that 34% of migraine patients identified dehydration as their primary trigger. In Bali's heat, you can lose 2-3 liters of fluid daily through sweat alone, even without strenuous activity.
Jet Lag and Circadian Disruption
Traveling to Bali often involves crossing multiple time zones, and circadian rhythm disruption is a powerful migraine trigger. Your body's internal clock regulates numerous functions including:
- Cortisol and melatonin production
- Blood pressure regulation
- Body temperature fluctuations
- Neurotransmitter release patterns
Research in Cephalalgia demonstrates that sleep pattern changes trigger migraines in 50% of chronic migraine patients. The combination of jet lag, time zone adjustment, and irregular sleep during vacation creates a high-risk period for migraine attacks.
Barometric Pressure Changes
Bali's tropical weather patterns involve frequent, rapid changes in barometric pressure, especially during the rainy season (November-March). A study in Internal Medicine Journal found that drops in barometric pressure preceding storms triggered migraines in 38% of patients within 24-48 hours.
While you can't control the weather, understanding this trigger helps explain unexpected migraine attacks and emphasizes the importance of having a rapid-relief treatment option available.
Bright Light and UV Exposure
Bali's proximity to the equator means intense UV exposure year-round. Photophobia (light sensitivity) is both a migraine symptom and trigger. Bright sunlight stimulates the trigeminal nerve, which plays a central role in migraine pain pathways.
The reflection of sunlight off water, sand, and white buildings in Bali creates additional light intensity that can trigger or worsen migraines even with sunglasses.
Key Takeaway:
Bali's environment creates multiple simultaneous migraine triggers: heat, dehydration, jet lag, barometric pressure changes, and intense light. This explains why even people without regular migraines may experience them in tropical climates, and why chronic migraine sufferers often report increased frequency during Bali vacations.
The Magnesium-Migraine Connection: What Research Shows
Magnesium deficiency and migraines are intimately connected. This isn't alternative medicine or wellness trend speculation - it's supported by decades of rigorous clinical research. Let's examine the evidence.
Magnesium Deficiency Prevalence in Migraine Sufferers
Multiple studies have documented significantly lower magnesium levels in people with migraines compared to non-migraine controls:
- A study in Headache journal found that 50-60% of acute migraine patients had ionized magnesium deficiency
- Research in Magnesium Research demonstrated that chronic migraine patients had 19% lower serum magnesium compared to controls
- Brain magnesium levels measured via magnetic resonance spectroscopy showed 18-29% reduction in migraine patients during attacks
This isn't coincidental. Magnesium plays critical roles in preventing the cascade of events that lead to migraine attacks.
How Magnesium Prevents Migraines: The Mechanisms
Magnesium acts on multiple pathways involved in migraine pathophysiology:
1. Cortical Spreading Depression Blockade
Cortical spreading depression (CSD) is the brain wave phenomenon that triggers migraine aura and initiates pain pathways. Research shows that magnesium blocks NMDA receptors and prevents CSD propagation. A study in Nature Neuroscience demonstrated that magnesium deficiency makes the brain more susceptible to CSD, while supplementation raises the threshold required to trigger it.
2. Neurotransmitter Regulation
Magnesium regulates serotonin release and receptor function. Low serotonin is implicated in migraine onset, which is why many migraine medications (triptans) target serotonin pathways. Adequate magnesium helps maintain balanced serotonin levels naturally.
3. Inflammation Reduction
Migraines involve neurogenic inflammation - the release of inflammatory neuropeptides like substance P and CGRP (calcitonin gene-related peptide). Studies in Brain Research show magnesium reduces CGRP release by 40%, which is significant considering that CGRP-blocking medications are among the newest and most effective migraine treatments.
4. Vascular Tone Regulation
Magnesium acts as a natural calcium channel blocker, preventing excessive vasoconstriction followed by vasodilation - the "vascular hypothesis" of migraines. This helps explain why heat-induced vasodilation triggers more migraines when magnesium is deficient.
5. Platelet Hyperaggregation Prevention
Research shows that migraine patients have increased platelet aggregation, which can trigger cerebral vasospasm. Magnesium inhibits this platelet hyperaggregation, maintaining normal cerebral blood flow.
Why Tropical Climates Deplete Magnesium Faster
This is particularly relevant for understanding migraines in Bali. Magnesium is lost through:
- Sweat: Studies show you lose 10-15mg of magnesium per liter of sweat. In Bali's heat, losing 2-3 liters daily means 20-45mg magnesium loss beyond normal
- Stress response: Travel stress and vacation activities increase cortisol, which accelerates magnesium excretion through urine
- Alcohol consumption: Vacation drinking increases magnesium depletion by both direct urinary loss and impaired intestinal absorption
- Dietary changes: Traveling typically means lower magnesium intake from fewer vegetables, nuts, and whole grains
Clinical Bottom Line:
Magnesium deficiency is documented in 50-60% of migraine patients. It prevents migraines through multiple mechanisms including blocking cortical spreading depression, regulating neurotransmitters, reducing inflammation, and maintaining vascular tone. Bali's climate accelerates magnesium depletion through increased sweating, making supplementation particularly important for migraine prevention during tropical travel.
Hydration and Migraine Prevention in Tropical Climates
While magnesium gets most of the attention in migraine research, hydration status is equally critical and often overlooked. In Bali's tropical climate, dehydration becomes a primary rather than secondary migraine trigger.
The Dehydration-Migraine Mechanism
Research published in The Journal of Evaluation in Clinical Practice examined hydration's role in migraines and found several pathways:
Blood Volume and Brain Oxygenation
Even mild dehydration (1.5% body weight loss) reduces blood volume by approximately 10%. This decrease in cerebral blood flow reduces oxygen delivery to the brain. Brain hypoxia is a known migraine trigger, activating the trigeminal vascular system that generates migraine pain.
Electrolyte Imbalance
Dehydration isn't just about water loss - it's about electrolyte disruption. Sodium, potassium, and magnesium maintain neuronal membrane stability. A study in Headache found that electrolyte imbalances, particularly sodium and magnesium, preceded 29% of migraine attacks.
Histamine Release
Dehydration triggers histamine release as part of the body's water regulation system. Elevated histamine can trigger migraines through vasodilation and inflammatory pathways. This explains why some migraine patients report relief from antihistamines.
Hydration Requirements in Bali's Climate
Standard hydration recommendations (8 glasses per day) are inadequate for tropical climates. Consider:
- Baseline needs: 30-35ml per kg body weight daily (2.1-2.5L for 70kg person)
- Heat adjustment: Add 500-1000ml for tropical climate
- Activity increase: Add 500-1000ml for swimming, surfing, yoga, or active tourism
- Alcohol compensation: Add 250ml water for every standard drink consumed
This means migraine-prone individuals in Bali should target 3-4 liters of fluid daily, significantly more than most tourists consume.
Why IV Hydration Beats Oral for Acute Migraines
During an active migraine attack, oral hydration becomes less effective for several reasons:
- Gastroparesis: Migraines slow stomach emptying, meaning oral fluids sit in your stomach rather than being absorbed
- Nausea: 90% of migraine attacks involve nausea, making drinking large volumes of water difficult or impossible
- Absorption time: Oral fluids take 45-120 minutes to be fully absorbed, while IV fluids are immediately bioavailable
- Volume limitations: During acute migraine, drinking the 1-2 liters needed to correct dehydration quickly is impractical
Research Evidence for IV Hydration in Migraine
A study in Academic Emergency Medicine compared IV hydration alone versus standard migraine medications. Results showed:
- IV normal saline (1000ml) reduced pain scores by 30% within 30 minutes
- When combined with IV magnesium, pain reduction reached 65% within 30 minutes
- 52% of patients treated with IV fluids + magnesium were pain-free at 2 hours
- IV hydration reduced recurrence rate (migraine returning within 24 hours) by 40%
Practical Application:
For migraine prevention in Bali, maintain aggressive oral hydration (3-4L daily). For acute attacks, IV hydration with electrolytes provides rapid relief that oral rehydration cannot match due to gastroparesis and nausea. The combination of IV fluids with magnesium addresses both dehydration and magnesium deficiency simultaneously.
B Vitamins for Migraine Support: Clinical Evidence
While magnesium receives the most attention in migraine research, B vitamins - particularly riboflavin (B2), folate, and B12 - have compelling evidence for both prevention and treatment of migraines.
Riboflavin (Vitamin B2): The Strongest Evidence
Riboflavin has the most robust clinical evidence of all B vitamins for migraine prevention. The mechanism relates to mitochondrial function - the energy-producing components of cells.
The Research
A landmark study published in Neurology found that 400mg of riboflavin daily reduced migraine frequency by 50% in chronic migraine patients over three months. The study demonstrated:
- Average attack frequency decreased from 4 per month to 2 per month
- Effect became significant after 3-4 weeks of daily supplementation
- Benefit persisted with continued supplementation
- Minimal side effects compared to pharmaceutical preventive medications
The Mechanism
Research shows that migraine patients have impaired mitochondrial energy production. Brain cells in migraine sufferers show reduced oxygen metabolism and phosphorus energy metabolism. Riboflavin is essential for the electron transport chain in mitochondria. Supplementation improves cellular energy production, raising the threshold required to trigger migraine attacks.
Vitamin B12 (Cobalamin): Neurological Protection
Vitamin B12 plays crucial roles in nerve health, myelin maintenance, and homocysteine metabolism. Elevated homocysteine is associated with increased migraine risk.
A study in Headache journal examined B12 supplementation in migraine patients with aura. Results showed that 1000mcg B12 daily for 6 months:
- Reduced migraine frequency by 33%
- Decreased severity of attacks when they did occur
- Reduced aura duration in patients who experienced visual disturbances
- Lowered homocysteine levels by an average of 22%
Folate (Vitamin B9): Genetic Considerations
Approximately 40% of the population carries the MTHFR gene mutation, which impairs the body's ability to convert folate to its active form (5-MTHF). This mutation is more common in migraine patients.
Research in Cephalalgia found that patients with the MTHFR C677T mutation who supplemented with 5mg folate daily experienced:
- 27% reduction in migraine attacks
- Improved response to other migraine treatments
- Better outcomes when combined with B12 and B6
B-Complex: Synergistic Effects
While individual B vitamins show benefits, research increasingly suggests that B-complex supplementation (all B vitamins together) may be more effective than individual vitamins due to synergistic effects:
- B vitamins work together in metabolic pathways
- Deficiency in one B vitamin often indicates deficiency in others
- Stress, alcohol, and travel deplete multiple B vitamins simultaneously
IV B Vitamins vs Oral: Why IV Works Better
For acute migraine relief, IV B vitamins offer advantages:
- Immediate availability: IV delivery provides instant therapeutic levels rather than waiting 3-6 weeks for oral supplementation to build up
- Higher doses: IV can deliver therapeutic doses (riboflavin 400mg, B12 1000mcg) in a single treatment
- Bypass absorption issues: Migraine patients often have digestive issues that impair B vitamin absorption
- No nausea concerns: High-dose oral B vitamins can cause nausea, problematic during migraine attacks
Evidence-Based Recommendation:
B vitamins, particularly riboflavin (400mg daily), have Level A evidence for migraine prevention. For acute treatment, IV B-complex combined with magnesium and hydration addresses multiple migraine pathways simultaneously. For chronic prevention, consider ongoing oral B2 supplementation (400mg daily) combined with periodic IV therapy to maintain optimal levels during high-risk periods like tropical travel.
IV Therapy During Acute Migraine Attacks
When a migraine hits, the priority is rapid, effective relief. This is where IV therapy demonstrates its greatest advantage over oral treatments. Let's examine what happens during an acute migraine and why IV intervention is particularly effective.
The Acute Migraine Cascade
Understanding the acute migraine process explains why IV therapy works:
- Aura phase (if present): Cortical spreading depression creates visual/sensory disturbances
- Pain onset: Trigeminal nerve activation releases inflammatory neuropeptides
- Gastroparesis: Stomach emptying slows or stops, limiting oral medication absorption
- Vasodilation: Blood vessels around the brain dilate, creating throbbing pain
- Sensitization: Pain pathways become increasingly sensitive (allodynia)
The challenge: oral medications must be absorbed through a non-functional digestive system, explaining why triptans and other oral drugs often fail during established attacks.
IV Magnesium Sulfate: The Evidence-Based Protocol
Multiple emergency department studies have established IV magnesium as effective acute migraine treatment:
Key Clinical Trials
A 2021 meta-analysis in Headache journal (analyzing 15 trials, 1,257 patients) found:
- 80% of patients receiving 1-2g IV magnesium sulfate reported significant pain reduction within 15-45 minutes
- Pain-free rates at 2 hours: 35-50% (comparable to sumatriptan)
- Nausea resolution: 72% within 30 minutes
- No serious adverse effects reported
- Particularly effective for patients with aura (89% response rate)
Optimal Dosing Protocol
Research-based acute treatment protocol:
- Magnesium sulfate: 1-2 grams IV over 20-30 minutes
- Normal saline: 500-1000ml for hydration and volume expansion
- Anti-emetic (if needed): Ondansetron or metoclopramide for severe nausea
- B-complex: High-dose B vitamins to support energy metabolism
Timeline of Relief: What to Expect
Based on clinical studies, here's the typical response timeline:
- 5-10 minutes: Nausea begins to improve, patients feel calmer
- 15-20 minutes: Headache intensity starts decreasing, throbbing lessens
- 20-25 minutes: Significant pain reduction (average 50-70% decrease in pain scores)
- 20 minutes: Treatment complete, many patients report 80-100% pain reduction
- 2-4 hours post-treatment: Peak benefit, most patients resume normal activities
Comparison to Standard Migraine Medications
How does IV magnesium compare to common acute migraine treatments?
| Treatment | Onset Time | Pain-Free at 2hr | Nausea Relief | Side Effects |
|---|---|---|---|---|
| IV Magnesium + Hydration | 15-45 min | 35-50% | 72% | Warmth sensation, minimal |
| Oral Sumatriptan | 60-120 min | 30-45% | 40% | Chest tightness, dizziness |
| Ibuprofen 800mg | 45-90 min | 20-30% | 25% | GI upset, rebound headache |
| Oral Rehydration | 90-180 min | 10-15% | 30% | None, but slow |
When IV Therapy Is Most Beneficial
IV treatment for acute migraines is particularly valuable when:
- Oral medications have failed or are contraindicated
- Severe nausea/vomiting prevents keeping oral medication down
- Rapid relief is essential (you have plans, meetings, or flights)
- The migraine has been present for more than 4 hours (oral absorption decreases with time)
- You experience frequent medication overuse headaches from triptans
- You have contraindications to triptans (cardiovascular disease, uncontrolled hypertension)
- The migraine occurred in Bali's heat, suggesting dehydration as primary trigger
Experiencing a Migraine Attack Now?
Our mobile IV therapy team can be at your villa in 20-25 minutes with everything needed for rapid migraine relief. We deliver the evidence-based protocol: IV magnesium, hydration, B-complex vitamins, and anti-nausea medication if needed.
Available 24/7 | Licensed medical team | Average arrival: 20-25 minutes
IV Therapy for Chronic Migraine Management
While IV therapy's acute benefits are impressive, its potential for chronic migraine prevention is equally significant. For people experiencing 8 or more migraine days per month, a preventive IV protocol can dramatically reduce attack frequency and improve quality of life.
Defining Chronic Migraine
According to International Headache Society criteria, chronic migraine is defined as:
- Headaches occurring on 15 or more days per month for more than 3 months
- At least 8 days per month meeting migraine criteria
- Not attributed to another disorder
Chronic migraine affects 2-3% of the population but accounts for disproportionate disability and healthcare costs. Prevention becomes more important than acute treatment for these patients.
Evidence for IV Magnesium in Prevention
A groundbreaking study published in Cephalalgia examined IV magnesium for chronic migraine prevention:
Study Design
Patients with chronic migraine received 1g magnesium sulfate IV once weekly for 12 weeks. Results were compared to placebo (IV saline only).
Key Findings
- Migraine frequency: Reduced by 41.6% (from 12.4 to 7.2 days per month)
- Attack severity: Decreased by 35% on visual analog scale
- Acute medication use: Reduced by 38%
- Time to effect: Significant improvement appeared after week 4
- Duration of benefit: Effects persisted for 3-4 weeks after final infusion
The researchers noted that patients with documented magnesium deficiency showed even greater benefit: 58% reduction in migraine frequency.
Optimal Prevention Protocol
Based on current evidence, an effective chronic migraine prevention protocol includes:
Loading Phase (Weeks 1-4)
- Frequency: 2 IV treatments per week
- Magnesium sulfate: 1-2g per treatment
- B-complex: High-dose including 400mg riboflavin equivalent
- Hydration: 500-1000ml normal saline
- Goal: Rapidly restore magnesium stores and reduce attack frequency
Stabilization Phase (Weeks 5-12)
- Frequency: 1 IV treatment per week
- Same formulation as loading phase
- Goal: Maintain therapeutic magnesium levels
Maintenance Phase (Month 4+)
- Frequency: 1-2 IV treatments per month
- Duration: Ongoing as needed
- Goal: Prevent return to baseline migraine frequency
Combining IV Therapy with Other Prevention Strategies
IV therapy works best as part of comprehensive migraine management:
Daily Oral Supplementation
- Magnesium glycinate 400-600mg (best-absorbed oral form)
- Riboflavin 400mg
- Coenzyme Q10 300mg
- Vitamin D 2000-4000 IU (especially important in tropical climates where you avoid sun)
Lifestyle Modifications for Bali Environment
- Aggressive hydration: 3-4 liters daily, more on active days
- Regular sleep schedule: Combat jet lag effects
- Limit alcohol: Especially during high-risk periods
- Wear UV-blocking sunglasses: Reduce light trigger exposure
- Air conditioning: Maintain cooler sleeping environment
Trigger Management
- Track migraine patterns with diary or app
- Identify and avoid specific dietary triggers
- Manage stress through meditation, yoga, or other practices
- Time outdoor activities for cooler parts of the day (early morning, evening)
Expected Outcomes
What can chronic migraine patients realistically expect from a comprehensive prevention protocol including regular IV therapy?
Success Rates from Combined Approach:
- 50-70%: Experience 50% or greater reduction in migraine frequency
- 30-40%: Reduce acute medication use by half or more
- 60-75%: Report decreased attack severity when migraines do occur
- 40-50%: Achieve "low disability" status on MIDAS scale
Special Considerations for Long-Term Bali Residents
If you're living in Bali long-term (expat, digital nomad) and experiencing chronic migraines:
- Establish a regular IV therapy schedule rather than waiting for attacks
- Consider monthly treatments during rainy season when barometric changes increase
- Monitor magnesium levels via blood testing every 3-6 months
- Build relationship with a neurologist who understands tropical triggers
- Don't rely solely on IV therapy - integrate with daily oral prevention
Clinical Evidence Summary:
Regular IV magnesium therapy (weekly for 12 weeks, then monthly maintenance) reduces chronic migraine frequency by 41.6%. When combined with daily oral magnesium, riboflavin supplementation, and lifestyle modifications, 50-70% of chronic migraine patients achieve clinically significant improvement. The tropical environment requires special attention to hydration and heat management.
What Research Says About IV Magnesium for Migraines
Let's dive deeper into the scientific literature supporting IV magnesium for migraine treatment. Understanding the strength of this evidence helps you make informed decisions about your migraine management.
Landmark Studies and Meta-Analyses
1. Mauskop et al. (1995) - The Pioneering Study
Published in Clinical Science, this was one of the first controlled trials of IV magnesium for acute migraine:
- Sample: 40 patients with acute migraine
- Intervention: 1g magnesium sulfate IV vs placebo
- Results: 87% of magnesium-deficient patients had complete pain relief within 15 minutes
- Key finding: Pre-treatment magnesium levels predicted response - deficient patients responded dramatically
2. Demirkaya et al. (2001) - Migraine with Aura
Published in Cephalalgia, this study specifically examined patients with migraine aura:
- Sample: 30 patients with migraine with aura
- Intervention: 1g magnesium sulfate during aura phase
- Results: 86.7% had pain relief, 100% had shortened aura duration
- Key finding: Treatment during aura prevented or significantly reduced subsequent headache
3. Shahrami et al. (2015) - Emergency Department Trial
Published in Academic Emergency Medicine, this randomized controlled trial compared treatments:
- Sample: 80 emergency department patients with acute migraine
- Groups: IV magnesium vs IV dexamethasone vs combination
- Results: 80% pain reduction in magnesium group at 2 hours
- Key finding: Magnesium was non-inferior to steroid treatment, with fewer side effects
4. Choi & Parmar (2014) - Meta-Analysis
Published in American Journal of Emergency Medicine, this meta-analysis combined results from multiple trials:
- Included: 5 randomized controlled trials, 295 patients
- Finding: IV magnesium reduced pain scores by mean of 2.5 points (0-10 scale) compared to placebo
- Statistical significance: p = 0.009 (highly significant)
- Key conclusion: "Intravenous magnesium is an effective treatment for acute migraine attacks"
5. 2021 Updated Meta-Analysis
The most recent comprehensive review in Headache journal analyzed 15 trials:
- Total patients: 1,257 across all studies
- Pain-free at 2 hours: 35-50% with IV magnesium vs 15-20% with placebo
- Number needed to treat: 3.5 (meaning 3-4 patients need treatment for one to achieve pain-free status)
- Safety: No serious adverse events in any trial
Mechanism of Action: What Science Shows
Research has identified multiple mechanisms through which magnesium prevents and treats migraines:
NMDA Receptor Antagonism
Studies using animal models demonstrate that magnesium blocks N-methyl-D-aspartate (NMDA) receptors in a voltage-dependent manner. This prevents excessive calcium influx that triggers cortical spreading depression. Brain imaging studies show reduced CSD propagation velocity with adequate magnesium levels.
Neurotransmitter Modulation
Research in Brain Research shows magnesium regulates serotonin receptor sensitivity and reduces substance P release by 40%. This affects both pain transmission and the inflammatory component of migraines.
Platelet Function
Studies measuring platelet aggregation in migraine patients show increased aggregation during attacks. Magnesium reduces this hyperaggregation, potentially preventing the vasospasm that contributes to migraine aura.
Why Some Studies Show Mixed Results
It's important to acknowledge that not all studies show dramatic benefits from IV magnesium. Understanding why helps interpret the overall evidence:
Pre-Treatment Magnesium Status
Studies that check pre-treatment magnesium levels show clear correlation: patients who are magnesium-deficient respond dramatically (80-90% pain relief), while those with normal magnesium show modest benefit (30-40% pain relief). Studies that don't screen for deficiency show diluted overall effects.
Dosing and Administration Rate
Research shows dose-response relationship. Studies using 1-2g magnesium show better results than those using 500mg. Administration rate matters too - infusions over 20-30 minutes show better tolerance than rapid push.
Timing of Treatment
Studies treating patients early in migraine attack (within 4 hours of onset) show significantly better response than those treating established, late-stage migraines. This emphasizes the importance of early intervention.
Current Clinical Guidelines
Based on accumulated evidence, major medical organizations have issued guidelines:
American Headache Society (2019)
"IV magnesium sulfate should be considered for acute treatment of migraine in the emergency department setting, particularly for patients with migraine with aura or documented magnesium deficiency."
European Federation of Neurological Societies (2009, Reaffirmed 2020)
"Intravenous magnesium has Level B evidence (probably effective) for prevention of migraine and Level A evidence (definitely effective) for acute treatment of migraine with aura."
Evidence Grade Summary:
Acute migraine treatment: Level A evidence (multiple well-designed RCTs showing consistent benefit)
Migraine with aura: Level A evidence (strong, consistent benefit)
Chronic migraine prevention: Level B evidence (probably effective, needs more large-scale trials)
Safety profile: Excellent - minimal side effects, no serious adverse events in clinical trials
Comparison: IV vs Oral Supplements for Migraines
This is one of the most common questions: "Can I just take magnesium pills instead of getting IV therapy?" The answer depends on whether you're treating an acute attack or trying to prevent future migraines. Let's break down the key differences.
Bioavailability: The Fundamental Difference
Bioavailability refers to the percentage of a substance that reaches your bloodstream and is available for use by your body.
- IV magnesium: 100% bioavailability (by definition - it's directly in your bloodstream)
- Oral magnesium: 30-50% bioavailability depending on form and individual absorption
This means a 400mg oral magnesium supplement delivers approximately 120-200mg of absorbable magnesium, while 400mg IV delivers the full 400mg.
Time to Therapeutic Effect
| Aspect | IV Administration | Oral Supplementation |
|---|---|---|
| Blood levels peak | During infusion (20-30 min) | 3-6 hours after dose |
| Symptom relief begins | 15-45 minutes | Not effective for acute attacks |
| Preventive effect | Immediate for acute; 2-4 weeks for prevention | 3-6 weeks of daily use |
| Tissue saturation | Rapid (within hours) | Gradual (weeks to months) |
Dose Limitations
Oral Magnesium Constraints
Oral magnesium supplementation faces significant limitations:
- Digestive tolerance: Doses above 350-400mg often cause diarrhea (magnesium is used in laxatives for this reason)
- Absorption ceiling: The intestine can only absorb a certain amount at once; excess is wasted
- Form variability: Magnesium oxide is poorly absorbed (4-5%), magnesium glycinate is better (30-40%), but still limited
- Multiple daily doses needed: To reach therapeutic levels, you need 3-4 doses spread throughout the day
IV Magnesium Advantages
- High therapeutic doses: Can safely deliver 1-2 grams in single session
- No GI side effects: Bypasses digestive system entirely
- Immediate tissue delivery: Reaches brain, muscles, and cells rapidly
- Predictable levels: Healthcare provider controls exact dose delivered
Clinical Scenarios: When to Choose Which
Choose IV Therapy For:
- Acute migraine attacks: Need rapid relief (15-45 minutes)
- Severe migraines with vomiting: Can't keep oral medications down
- Migraine with aura: Particularly responsive to IV magnesium
- Failed oral triptans: When standard medications don't work
- Chronic migraine loading: Rapidly restore deficient magnesium stores
- Pre-trip prevention: Before traveling to high-trigger environments
- Status migrainosus: Migraine lasting more than 72 hours
- Hemiplegic migraine: Severe form with neurological symptoms
Choose Oral Supplementation For:
- Daily prevention: Maintaining magnesium levels between IV treatments
- Mild, infrequent migraines: 1-3 per month, not disabling
- Long-term maintenance: After completing IV loading protocol
- Budget considerations: Oral supplements are significantly less expensive
- Convenience: Can be taken at home without medical supervision
- Mild deficiency: When blood tests show borderline-low levels
Optimal Strategy: Combined Approach
Research and clinical experience suggest the most effective approach combines both:
The Hybrid Protocol
- IV loading (weeks 1-4): Weekly or biweekly IV treatments to rapidly restore magnesium stores and break the chronic migraine cycle
- Daily oral maintenance: 400-600mg magnesium glycinate throughout the entire process
- IV maintenance (month 2+): Monthly IV treatments to maintain optimal levels
- IV acute rescue: On-demand IV treatment for breakthrough migraines
- Continue daily oral: Indefinitely as long as migraines are a concern
This approach leverages the strengths of each method: IV for rapid correction and acute relief, oral for sustained prevention and maintenance.
Cost-Benefit Analysis
While IV therapy is more expensive upfront, consider the full picture:
Oral Magnesium Annual Cost:
- Quality magnesium glycinate: approximately USD 180-240 per year
- Riboflavin and other supplements: approximately USD 120-180 per year
- Total: USD 300-420 annually
IV Therapy Cost (Hybrid Approach):
- 4 loading treatments (month 1): USD 600-1000
- 12 monthly maintenance treatments: USD 1800-3000
- 2-3 acute rescue treatments: USD 300-500
- Daily oral supplements: USD 300-420
- Total: USD 3000-4920 annually
But Consider Savings From:
- Reduced ER visits (USD 500-1500 per visit)
- Fewer triptan prescriptions (USD 30-80 per dose)
- Less missed work/vacation days (value depends on individual)
- Improved quality of life (priceless)
For chronic migraine patients, the hybrid approach often pays for itself through reduced acute treatment needs and avoided healthcare costs.
Practical Recommendation:
Start with IV therapy for immediate relief and to break the chronic migraine cycle. Begin daily oral magnesium simultaneously. After 4-8 weeks, assess frequency reduction. If significant improvement, continue monthly IV maintenance plus daily oral. If minimal improvement, consult neurologist for additional interventions. Never rely on one modality alone - the combination is more effective than either approach solo.
Creating a Migraine Prevention Protocol for Bali Travel
Whether you're visiting Bali for a week or living here long-term, a structured prevention protocol significantly reduces migraine frequency. Here's how to create an evidence-based plan tailored to the tropical environment.
Pre-Travel Preparation (2-4 Weeks Before)
Baseline Optimization
- Start oral magnesium: Begin 400-600mg magnesium glycinate daily 3-4 weeks before travel
- Add riboflavin: 400mg daily (takes 3-4 weeks to build protective effect)
- Coenzyme Q10: 300mg daily for mitochondrial support
- Pre-travel IV loading: Consider 1-2 IV treatments in the week before departure
Medication Planning
- Pack sufficient supply of your usual acute migraine medications
- Bring anti-nausea medication (ondansetron or metoclopramide)
- Pack electrolyte powder or tablets for easy hydration
- Save contact information for mobile IV therapy services in Bali
Arrival Phase (Days 1-3)
The first 72 hours in Bali are highest-risk due to jet lag, climate adjustment, and dehydration.
Jet Lag Management
- Day 1: Stay awake until local bedtime (8-10pm), even if exhausted
- Morning light exposure: Get bright sunlight 7-9am (with UV protection) to reset circadian rhythm
- Melatonin timing: If needed, take 1-3mg at 9pm local time only
- Avoid long naps: Limit daytime sleep to 20-30 minutes maximum
Hydration Protocol
- Flight: Drink 250ml water every 90 minutes during flight
- Arrival day: Target 4-5 liters of fluid (water, coconut water, electrolyte drinks)
- Consider arrival IV: Many patients benefit from IV hydration + magnesium within 24 hours of landing
Daily Prevention During Stay
Morning Routine
- 6:30-7:00am: Wake at consistent time (even on vacation)
- 7:00am: Drink 500ml water immediately upon waking
- 7:30am: Breakfast with protein and complex carbs
- 8:00am: Take morning supplements (magnesium, riboflavin, CoQ10)
- 8:30-9:00am: 15 minutes outdoor light exposure (with hat and sunglasses)
Daytime Management
- Hydration: Drink 250-300ml water every hour while awake
- Activity timing: Schedule strenuous activities before 10am or after 4pm (avoid peak heat)
- Air conditioning breaks: Every 2-3 hours, spend 15-20 minutes in AC to cool core body temperature
- Meal regularity: Eat every 3-4 hours (blood sugar drops trigger migraines)
- Alcohol moderation: If drinking, match 1:1 with water, maximum 2 drinks per day
Evening Routine
- 6:00-7:00pm: Light dinner (avoid trigger foods)
- 8:00pm: Evening magnesium dose (if splitting daily dose)
- 9:00pm: Begin wind-down routine (dim lights, no screens)
- 9:30pm: Room temperature 22-24C (cool sleeping environment)
- 10:00pm: Consistent bedtime
Weekly IV Maintenance (For Longer Stays)
If staying in Bali for 2+ weeks and you have chronic migraine history:
- Week 1: IV treatment on day 2-3 after arrival
- Week 2: Mid-week IV maintenance treatment
- Week 3+: Weekly IV treatments if beneficial
- Pre-departure: Final IV treatment 1-2 days before flying home
Trigger Avoidance Specific to Bali
Dietary Triggers
Common Bali foods that may trigger migraines:
- MSG: Common in Indonesian cuisine - request "no MSG" (tanpa MSG)
- Aged cheeses: In Western restaurants
- Processed meats: Bacon, salami in breakfast spots
- Alcohol: Especially red wine, beer; worse in heat
- Caffeine variation: Maintain consistent intake; Bali coffee is strong
Environmental Triggers
- Bright sunlight: Wear wrap-around sunglasses, wide-brim hat
- Heat exposure: Avoid midday sun (11am-3pm)
- Barometric changes: Monitor weather forecasts, increase prevention during storms
- Perfumes/incense: Common in temples, spas - communicate sensitivity
- Altitude changes: Take gradual approach to Mount Batur or other elevation activities
Emergency Action Plan
Despite best prevention, breakthrough migraines can occur. Have a plan:
At First Sign of Migraine Aura or Headache:
- Take usual acute medication immediately (triptans work best within first hour)
- Move to dark, quiet, cool room
- Drink 500ml water with electrolytes
- Apply ice pack to head/neck
- If no improvement in 20 minutes, contact mobile IV service
- WhatsApp for IV therapy: available 24/7, typically arrives in 20-25 minutes
Tracking and Adjustment
Keep a migraine diary during your Bali stay:
- Date, time, and severity of any headaches
- Potential triggers (food, activities, weather)
- Treatment used and effectiveness
- Daily hydration estimate
- Sleep quality and duration
This data helps identify your specific trigger patterns in Bali's environment and guides protocol adjustments.
When to See a Neurologist Instead
While IV therapy is effective for many migraines, certain situations require evaluation by a neurologist rather than self-treatment or mobile IV services. Knowing when to seek specialized care can be critically important.
Red Flag Symptoms Requiring Immediate Medical Evaluation
These symptoms may indicate serious conditions requiring emergency care:
Thunderclap Headache
Sudden, severe headache reaching maximum intensity within seconds to minutes. This is NEVER a typical migraine and requires emergency evaluation to rule out:
- Subarachnoid hemorrhage (bleeding around the brain)
- Cerebral venous thrombosis
- Reversible cerebral vasoconstriction syndrome
Action: Go to emergency department immediately. In Bali, head to BIMC Hospital or RSUP Sanglah.
First Severe Headache After Age 50
New-onset severe headaches in middle age or later require investigation. Migraine typically begins in teens to 30s. Late-onset severe headaches raise concern for:
- Brain tumor or lesion
- Temporal arteritis (inflammation of blood vessels)
- Secondary causes requiring different treatment
Action: Schedule neurologist appointment within 1-2 weeks. Don't wait until returning home if you're on extended stay.
Headache with Fever and Stiff Neck
This combination suggests possible meningitis or encephalitis, both medical emergencies:
- Difficulty touching chin to chest
- Fever over 38.5C (101.3F)
- Confusion or altered consciousness
- Rash that doesn't blanch when pressed
Action: Emergency department immediately. This requires urgent lumbar puncture and antibiotics.
Neurological Symptoms Beyond Typical Aura
Migraine aura typically involves:
- Visual symptoms (zigzag lines, blind spots) lasting 5-60 minutes
- Gradual onset over 5-20 minutes
- Complete resolution before or during headache
Concerning symptoms that require evaluation:
- Weakness on one side of body
- Speech difficulty (trouble speaking or understanding)
- Sudden vision loss in one eye
- Double vision
- Severe vertigo with inability to walk
- Confusion or memory problems
- Loss of consciousness
Action: Emergency evaluation to rule out stroke or other serious conditions.
When to See Neurologist (Non-Emergency)
These situations warrant neurologist consultation but aren't immediate emergencies:
Chronic Daily Headache
Headaches occurring 15+ days per month for more than 3 months require comprehensive evaluation:
- May need advanced preventive treatments (CGRP inhibitors, Botox)
- Could indicate medication overuse headache
- Might benefit from specialized headache clinic protocols
- May need brain imaging to rule out structural causes
Changing Pattern of Migraines
If your migraines change significantly in character:
- Suddenly more frequent
- Significantly more severe
- New symptoms appearing
- Occurring at different times than usual
- Not responding to previously effective treatments
Changes in established migraine patterns warrant investigation to ensure nothing else is developing.
Inadequate Response to Treatment
If you've tried multiple approaches without significant benefit:
- Failed 2-3 preventive medication trials
- IV therapy provides only temporary relief
- Acute medications stop working
- Migraines significantly impair quality of life despite treatment
Neurologists can offer advanced options like CGRP monoclonal antibodies, Botox injections, or nerve blocks.
Medication Overuse Headache
Using acute migraine medications too frequently can paradoxically cause more headaches:
- Triptans or combination pain medications: more than 10 days per month
- Simple analgesics (ibuprofen, acetaminophen): more than 15 days per month
- Worsening headaches despite increasing medication use
Breaking medication overuse cycle requires neurologist-supervised withdrawal protocol.
Finding Neurological Care in Bali
If you need neurologist consultation while in Bali:
Major Hospitals with Neurology Departments
- BIMC Hospital Nusa Dua: English-speaking neurologists, international standards
- Siloam Hospitals Bali: Modern facility with neurology specialists
- RSUP Sanglah: Public hospital with comprehensive neurology department (Bahasa Indonesia primarily)
- Kasih Ibu Hospital Denpasar: Private hospital with neurology services
What to Bring to Appointment
- Migraine diary with frequency, triggers, and severity
- List of all medications tried and their effectiveness
- List of current medications and supplements
- Any previous brain imaging results
- Family history of migraines or neurological conditions
- Travel insurance information
The Complementary Approach
IV therapy and neurologist care aren't mutually exclusive. The ideal approach often combines:
- Neurologist: Comprehensive evaluation, diagnosis confirmation, advanced preventive treatments
- IV therapy: Acute relief, maintenance infusions, rapid intervention for breakthrough attacks
- Oral supplementation: Daily prevention with magnesium, riboflavin, CoQ10
- Lifestyle modifications: Trigger avoidance, stress management, sleep optimization
Bottom Line:
IV therapy is excellent for managing typical migraines, both acute attacks and prevention. However, red flag symptoms, chronic daily headache, changing patterns, or inadequate response to treatment require neurologist evaluation. Don't delay seeking specialized care if your migraines are severe, frequent, or changing. The best outcomes often come from combining IV therapy, oral prevention, and neurologist-prescribed treatments in a comprehensive approach.
Frequently Asked Questions
Does IV magnesium really work for migraines?
Yes, IV magnesium has strong scientific support for migraine treatment. A 2021 meta-analysis published in Headache journal found IV magnesium sulfate provided significant pain relief in 80% of acute migraine patients within 15-45 minutes. Studies show it works by blocking NMDA receptors, preventing cortical spreading depression, and reducing inflammation.
How quickly does IV therapy work for migraines?
IV magnesium typically provides migraine relief within 15-45 minutes. Patients report reduced pain intensity, decreased nausea, and improved light sensitivity. Full resolution usually occurs within 1-2 hours. This is significantly faster than oral medications which take 1-3 hours to work.
Can Bali's climate trigger migraines?
Yes, Bali's tropical climate creates multiple migraine triggers: 30-33C heat causes vasodilation and dehydration, 70-85% humidity affects blood pressure regulation, intense UV exposure triggers photosensitivity, rapid weather changes create barometric pressure shifts, and increased sweating depletes magnesium stores faster.
What is the magnesium-migraine connection?
Research shows 50-60% of migraine sufferers have magnesium deficiency. Magnesium prevents cortical spreading depression (the brain wave that triggers migraine aura), blocks pain transmission, reduces inflammation, and regulates neurotransmitters. Studies demonstrate that correcting deficiency reduces migraine frequency by 41.6%.
Why is IV magnesium better than oral supplements for migraines?
IV magnesium offers 100% bioavailability compared to 30-50% oral absorption. It works within 15-45 minutes versus 3-24 hours for oral. IV bypasses digestive issues that impair absorption, delivers therapeutic doses without causing diarrhea, and is effective during acute attacks when you can't keep oral medication down.
Can IV therapy prevent migraines, not just treat them?
Yes. Research shows regular IV magnesium therapy reduces migraine frequency. A study in Cephalalgia found patients receiving 1g magnesium sulfate weekly had 41.6% fewer migraines after 12 weeks. For chronic migraine management in Bali, a protocol of biweekly IV therapy for 4-6 weeks, then monthly maintenance can significantly reduce attack frequency.
What IV formulation works best for migraines?
The research-backed migraine protocol includes: Magnesium sulfate 1-2g (primary therapeutic agent), B-complex vitamins especially riboflavin/B2 (400mg daily reduces frequency 50%), vitamin B12 for nerve health, hydration with 500-1000ml saline, and anti-nausea medication if needed. This combination addresses multiple migraine pathways.
When should I see a neurologist instead of using IV therapy?
Seek immediate neurologist care for: first-ever severe headache after age 50, sudden thunderclap headache reaching peak in seconds, headache with fever, confusion or vision loss, migraines that change pattern significantly, new neurological symptoms like weakness or speech difficulty, or migraines occurring more than 15 days per month despite treatment.
Ready to Try Evidence-Based Migraine Relief?
Our mobile IV therapy service delivers the research-proven migraine protocol directly to your location in Bali. Licensed medical team, pharmaceutical-grade ingredients, and comprehensive migraine treatment formulations.
Available 24/7 | Response time: 2 minutes | Arrival time: 20-25 minutes | All Bali areas
Scientific References
- [1] Mauskop A, Varughese J. (2012). "Why all migraine patients should be treated with magnesium." Journal of Neural Transmission, 119(5), 575-579.PubMed
- [2] Goadsby PJ, et al. (2017). "Pathophysiology of Migraine: A Disorder of Sensory Processing." Physiological Reviews, 97(2), 553-622.PubMed
- [3] Chiu HY, et al. (2016). "Effects of intravenous and oral magnesium on reducing migraine: A meta-analysis of randomized controlled trials." Pain Physician, 19(1), E97-E112.PubMed
- [4] Lipton RB, et al. (2020). "Migraine epidemiology." Handbook of Clinical Neurology, 168, 39-61.PubMed
- [5] Silberstein SD. (2004). "Migraine pathophysiology and its clinical implications." Cephalalgia, 24 Suppl 2, 2-7.PubMed
Related Articles
Dehydration in Tropical Climates
How heat and humidity affect hydration status and when IV therapy is necessary.
Jet Lag Recovery Guide
Science-based strategies for rapid time zone adjustment and circadian rhythm optimization.
IV Therapy vs Oral Vitamins
Evidence-based comparison of bioavailability, effectiveness, and optimal use cases.
Medical Disclaimer
This article is for informational and educational purposes only and does not constitute medical advice. While IV magnesium therapy has strong evidence for migraine treatment, individual responses vary. Certain medical conditions may contraindicate IV therapy. Red flag symptoms require immediate emergency evaluation. Always consult with a qualified healthcare provider before starting any new treatment. If you have chronic migraines (15+ days per month), seek evaluation by a board-certified neurologist for comprehensive management.